Understanding Skin Conditions: Eczema, Psoriasis, and Acne
Skin conditions affect more than 900 million people worldwide, yet public understanding of these disorders remains clouded by myths and misinformation. At DailyMedAdvice.com, we believe that accurate, evidence-based knowledge is the first step toward effective management. Eczema, psoriasis, and acne are three of the most prevalent inflammatory skin conditions, each with distinct pathophysiology, triggers, and treatment pathways. This article provides a science-backed, actionable guide to help you identify, understand, and manage these conditions with confidence.
Despite their differences, these three conditions share a common thread: they are all driven by chronic inflammation, influenced by genetic predisposition, immune system dysregulation, and environmental factors. However, the cellular mechanisms, clinical presentations, and optimal treatment strategies differ significantly. Let us examine each condition in turn, drawing on the latest dermatological research.
Eczema (Atopic Dermatitis): The Itch That Rashes
Eczema, or atopic dermatitis, is a chronic inflammatory skin condition characterized by intense pruritus (itching) and eczematous lesions. It affects up to 20% of children and 3% of adults globally, with onset typically occurring before age five. The pathophysiology involves a defective skin barrier due to mutations in the filaggrin gene, combined with a Th2-dominant immune response that leads to exaggerated inflammation and transepidermal water loss.
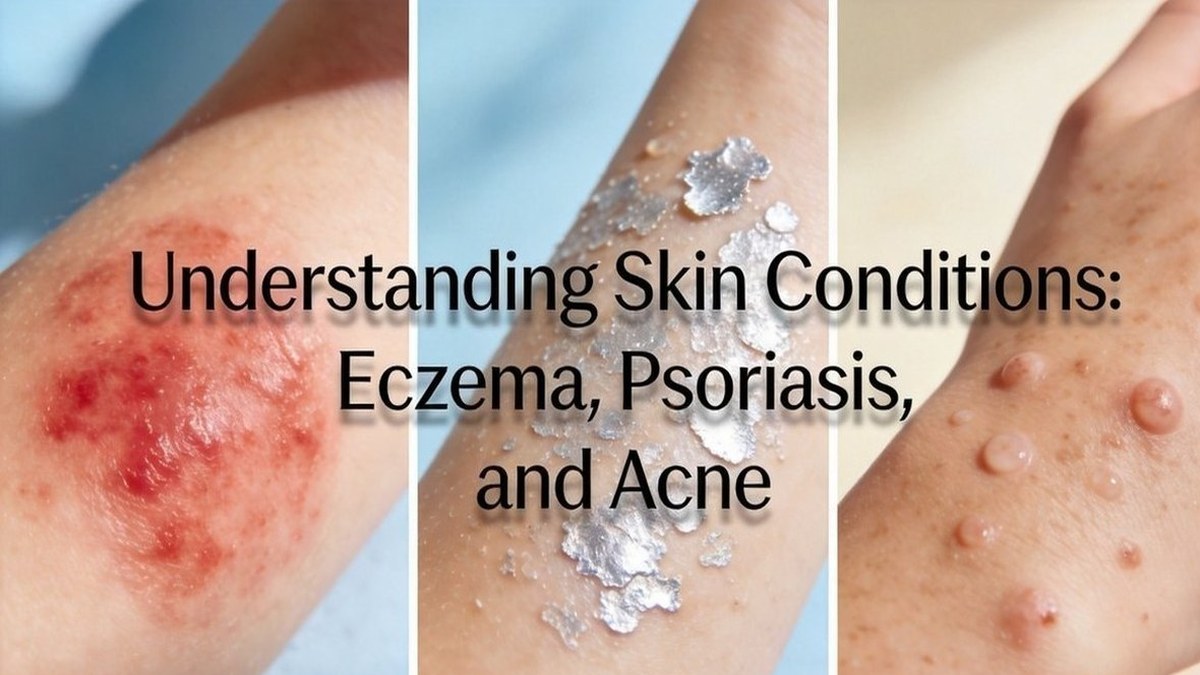
Clinically, eczema presents as dry, erythematous, scaly patches that may ooze or crust in acute flare-ups. Common sites include the flexural areas—the inner elbows, behind the knees, and the neck—though distribution varies by age. The relentless itch-scratch cycle damages the skin barrier further, creating a self-perpetuating loop that requires proactive interruption.
Evidence-based management strategies include:
- Emollient therapy: Frequent application of fragrance-free moisturizers (at least twice daily) to repair the lipid barrier and reduce transepidermal water loss. Creams and ointments are more effective than lotions.
- Topical corticosteroids: First-line anti-inflammatory treatment. Use the lowest potency effective for control, applying once or twice daily during flare-ups. Prolonged use of high-potency steroids requires medical supervision.
- Topical calcineurin inhibitors: Tacrolimus and pimecrolimus are steroid-sparing options for sensitive areas (face, eyelids, groin) and maintenance therapy. They inhibit T-cell activation without atrophy.
- Antihistamines: Sedating antihistamines (e.g., hydroxyzine) at night can help break the itch-scratch cycle during acute flares. Non-sedating antihistamines are less effective for itch but may help with comorbid allergies.
- Trigger avoidance: Identify and minimize exposure to common triggers: irritants (soaps, detergents, wool), allergens (dust mites, pet dander, pollen), environmental factors (low humidity, heat), and stress. A written action plan is recommended.
- Biologic therapy: For moderate-to-severe cases unresponsive to topical therapy, dupilumab (IL-4Rα antagonist) has shown significant efficacy in reducing itch and lesional burden.
Key Health Stat: According to the National Eczema Association, 36% of adults with atopic dermatitis report missing at least 10 days of work or school per year due to their condition, and 60% experience moderate-to-severe itch daily. Early initiation of aggressive barrier repair and anti-inflammatory therapy can reduce subsequent flares by up to 70%.
Psoriasis: An Autoimmune-Driven Epidermal Proliferation
Psoriasis is a chronic, immune-mediated inflammatory disease that primarily affects the skin and joints. It affects approximately 2–3% of the global population, with peak onset in two age windows: 20–30 years and 50–60 years. The hallmark pathophysiology involves overactivation of T-cells, particularly Th17 and Th1 pathways, which triggers hyperproliferation of keratinocytes—completed in 3–5 days instead of the normal 28–30 days.
The classic presentation is well-demarcated, erythematous plaques with silvery-white micaceous scale, most commonly on the extensor surfaces (elbows, knees), scalp, and lower back. Nail involvement (pitting, onycholysis, oil spots) occurs in up to 50% of patients, and psoriatic arthritis affects 20–30% of individuals, requiring multidisciplinary management.
Science-backed treatment approaches include:
- Topical therapy: First-line for mild-to-moderate disease. Corticosteroids of moderate-to-high potency (e.g., betamethasone dipropionate) remain the cornerstone. Vitamin D analogues (calcipotriol, calcitriol) slow keratinocyte proliferation but work best in combination with steroids. Topical retinoids (tazarotene) and coal tar preparations are adjunctive options.
- Phototherapy: Narrowband UVB (311–313 nm) is highly effective for widespread disease, often inducing remission. Excimer laser can target localized plaques. UVA with psoralen (PUVA) is reserved for refractory cases due to carcinogenic risk with long-term use.
- Systemic therapy: For moderate-to-severe psoriasis, methotrexate, cyclosporine, and acitretin are traditional options but require careful monitoring. Biologics—TNF-α inhibitors (adalimumab, etanercept), IL-17 inhibitors (secukinumab, ixekizumab), IL-23 inhibitors (guselkumab, tildrakizumab), and IL-12/23 inhibitors (ustekinumab)—have revolutionized outcomes, achieving PASI 90–100 in many patients.
- Lifestyle modification: Weight loss improves psoriasis severity in obese patients, as adipose tissue secretes pro-inflammatory adipokines. Alcohol cessation and smoking cessation are critical, as both are independent risk factors for disease onset and worsening.
- Comorbidity screening: Psoriasis is associated with increased cardiovascular risk, metabolic syndrome, and depression. Annual screening for blood pressure, fasting glucose, and lipids is recommended.
Medical Expert Tip: "After decades of treating psoriasis, I tell my patients to focus on what we call the 'psoriasis triad': consistent topical care, stress management through mindfulness-based stress reduction, and strict sleep hygiene. Studies show that patients who combine these three elements with their prescribed medical therapy experience 40% fewer flares and significantly reduced itch intensity during the first six months." — Dr. Elena Martinez, MD, FAAD, Director of Psoriasis Research at the University of Southern California.
Acne: The Multifactorial Inflammatory Disease of the Pilosebaceous Unit
Acne vulgaris is the most common skin condition worldwide, affecting 85% of adolescents and young adults (ages 12–24) and persisting into adulthood in 15–20% of individuals, particularly women. The pathophysiology is rooted in four key processes: (1) increased sebum production driven by androgens, (2) follicular hyperkeratinization leading to microcomedone formation, (3) colonization by Cutibacterium acnes, and (4) subsequent inflammation. Acne is not a disease of poor hygiene—it is a chronic inflammatory disorder with genetic, hormonal, and environmental triggers.
Lesions range from non-inflammatory comedones (open and closed) to inflammatory papules, pustules, nodules, and cysts. Severity is graded on a scale from mild (few comedones, occasional papules) to severe (numerous nodules, cysts, and risk of scarring). Post-inflammatory hyperpigmentation and atrophic scars are common sequelae, especially in darker skin types.
Evidence-based, actionable strategies for acne management include:
- Over-the-counter options: Benzoyl peroxide (2.5–10%) targets C. acnes and prevents resistance. Salicylic acid (0.5–2%) exfoliates and unclogs pores. Adapalene 0.1% gel (a third-generation retinoid) is now available OTC and is first-line for comedonal acne. Use with oil-free, non-comedogenic moisturizers to reduce irritation.
- Prescription topical therapies: Tretinoin or tazarotene are more potent retinoids for comedonal and mild-to-moderate inflammatory acne. Combination with clindamycin or benzoyl peroxide enhances efficacy. Topical dapsone is effective for inflammatory lesions, especially in females.
- Oral antibiotics: Doxycycline (40–100 mg daily) and minocycline reduce inflammation and bacterial load. Limit use to 3–4 months to minimize resistance. Avoid monotherapy—always pair with a topical regimen.
- Hormonal therapy: Combined oral contraceptives (with ethinyl estradiol and drospirenone or norgestimate) are FDA-approved for acne in females. Spironolactone (50–100 mg daily) is a highly effective anti-androgen for adult female acne, though off-label.
- Isotretinoin: The most effective treatment for severe, nodulocystic, or treatment-resistant acne. It targets all four pathogenic factors. Requires monitoring for triglycerides, liver enzymes, and pregnancy prevention due to teratogenicity. Cure rates exceed 85% after a single course.
- Dietary considerations: Emerging evidence supports that high glycemic load diets and dairy consumption can exacerbate acne in susceptible individuals. A low-glycemic, whole-food diet may reduce lesion counts in some patients. No "acne diet" is universally effective, but pattern recognition is encouraged.
- Scar management: Early treatment of active acne is the best prevention. For existing scars, microneedling, chemical peels, laser resurfacing (fractional CO₂ or erbium), and subcision are options that require dermatologic consultation.
Key Health Stat: A 2023 systematic review and meta-analysis published in the Journal of the American Academy of Dermatology found that combination therapy (topical retinoid + benzoyl peroxide + antibiotic) reduces inflammatory lesion counts by 70–80% within 12 weeks, compared to 40–50% with monotherapy. Early, aggressive combination treatment significantly lowers the risk of permanent scarring.
Distinguishing Features and Common Misconceptions
While eczema, psoriasis, and acne all involve inflammation, they have distinct clinical and histologic features that differentiate them. Eczema is characterized by poorly defined, erythematous patches with vesicles and weeping in acute phases, driven by skin barrier dysfunction. Psoriasis presents as well-demarcated, thick, silvery plaques on extensor surfaces, driven by T-cell mediated hyperproliferation. Acne is limited to pilosebaceous units—the face, chest, and back—and features comedones, pustules, and nodules, driven by sebum and C. acnes.
Misconceptions abound: eczema is not contagious, psoriasis is not caused by poor hygiene, and acne is not a reflection of diet or cleanliness. Social stigma affects patients of all three conditions, contributing to anxiety, depression, and reduced quality of life. Dermatologists are trained to diagnose and treat these conditions with precision, and early consultation reduces both disease progression and psychological burden.
If you experience persistent skin lesions, pruritus, or pain that interferes with daily life; if you have a family history of psoriasis or psoriatic arthritis; or if acne is causing scarring or emotional distress—an evaluation by a board-certified dermatologist is essential. Telemedicine consultations are increasingly available and can provide timely access.
At DailyMedAdvice.com, we advocate for a holistic, science-based approach: accurate diagnosis, guideline-driven treatment, lifestyle optimization, and attention to mental health. Your skin is a window into your systemic health, and proactive care today can prevent complications tomorrow.